

Pressure ulcer litigation: Prevention is better than cure
The NHS has spent a staggering £168 million on litigation claims in relation to pressure ulcers since 2013.1 With pressure ulcers being a common challenge across healthcare facilities, the figure illustrates potentially significant cost savings for many hospitals at a time where budget management is critical. How can we support each other to reverse this trend, avoid the additional workload that litigation can entail and increase staff confidence?
Sizing up the impact
When calculating the impact of hospital-acquired pressure ulcers (HAPUs), we often look at the cost of PU treatment and the impact on length of stay. But these new figures suggest that the true cost of a HAPU may not have been fully understood until now.
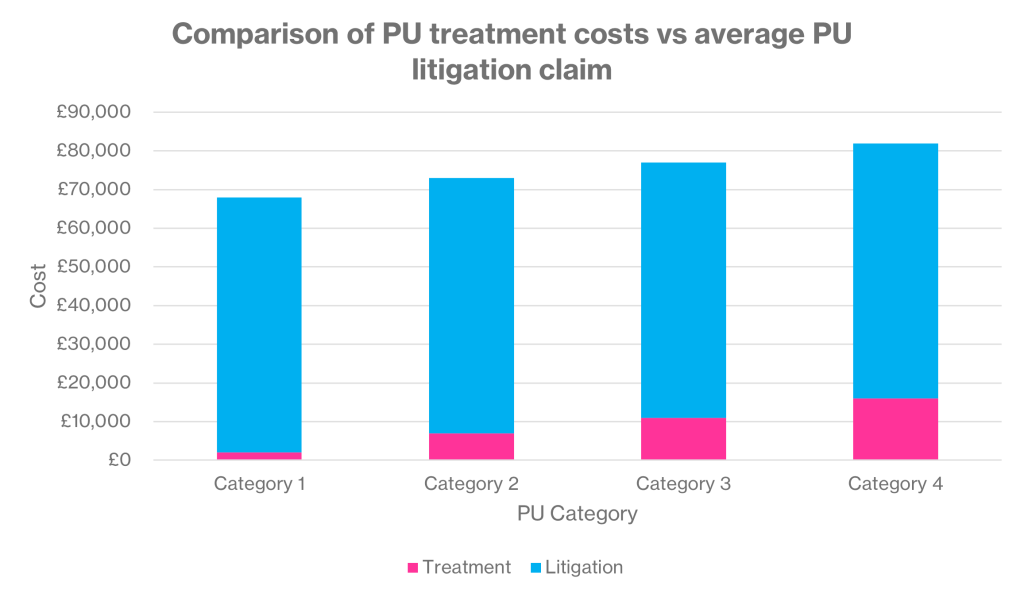
According to a Freedom of Information (FOI) request, the NHS spent over £16 million in the last financial year on 254 pressure ulcer-related claims.2 This works out to an average cost of roughly £66,000 per claim. Compared to the estimated treatment costs for each category of pressure ulcer (PU), as set out in the NHS’ PU productivity calculator, the difference is stark (see Figure 1).
And more HAPU claims are resolved with compensation compared to other clinical claims. Over an eight-year period, 91% of HAPU-related claims resulted in payouts, totalling £126.5 million. By comparison, only 66% of clinical claims overall were closed with compensation payments (2020/21).4
Effects on staff
But the impact of litigation on the NHS goes beyond pure financials. There’s a huge emotional impact. Litigation can hit morale, increase stress and knock staff confidence.5,6
“If something has happened, whether they [staff] were on duty or not, it really affects staff morale”. – Maria Caulfield, Former Minister of State for Health, on incident investigation.7
One study assessed how being involved in a litigation claim affected healthcare professionals, with the result that some considered taking time off sick or even leaving the profession entirely.8 At a time where recruitment and retention are key issues for the NHS, the impact of litigation can’t be overlooked.

Preventative action is key
As busy clinicians, it’s easy to react when a problem has occurred, instead of taking a step back and looking at a preventative approach. To help turn reactiveness into proactiveness, we’ve listed 5 top tips.
#1 Understand and identify at-risk patients
All patients are potentially at risk of developing a pressure ulcer, but some patients are more at risk than others. These include patients with:
- Significantly limited mobility
- Significant loss of sensation
- A previous or current pressure ulcer
- Significant cognitive impairment
- The inability to reposition themselves
- Nutritional deficiency10
#2 Examine your protocols
Are there steps you could take to make product selection easier? For example, a ‘long lie’ patient who has been immobile for several hours is at extremely high risk of developing a pressure ulcer (if they have not already). Upon hospital admission, it may be preferable to put them straight onto a higher-specification surface than normal. This can help to protect against pressure ulcers forming or increasing in severity.
#3 Review your available products
Are there additional products that could help? Consider a patient who is unable to reposition independently, and is therefore at a much higher risk of developing a PU. We can’t control the patient’s ability to reposition, but we can control what we put underneath them. This could be a higher-specification surface that may allow for reduced turning frequency, or a bed with lateral tilt functionality to help redistribute pressure.
Will this affect existing supplier contracts? Due to their specialist nature, advanced technologies such as Negative Pressure Wound Therapy (NPWT) or fluid-immersion simulation often fall outside of standard procurement contracts. As a result, these products are highly accessible in both hospital and community settings and can be safely added-on outside of your existing supply contract. Opting for a rental arrangement is often best when working with specialist equipment. Renting offers greater flexibility and allows additional products to be brought in as and when they’re required for particular patients.

#4 Audit your equipment
Old, suboptimal dynamic mattresses or bottomed-out foams increase pressure ulcer risks. To mitigate these, the CQC requires providers to make sure that equipment is properly used and maintained, and meets the latest regulatory standards.11 Regular, structured audits are key to ensuring this happens.
#5 Keep patients informed and involved
Patients are increasingly becoming more involved in decision making processes. Where they have the capacity to understand their pressure ulcer risk, getting them on board can help ease burden on nursing staff, improve compliance and benefit outcomes. Ensure patient resources are easy-to read with minimal jargon. Consider providing large print, Braille, signed or video versions.
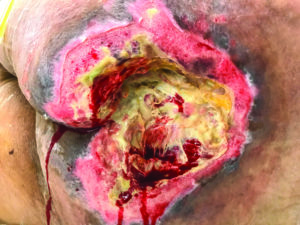
Each claim is a patient’s story
Most importantly, behind each pressure ulcer litigation claim is a patient. The impact of living with a pressure ulcer cannot be underestimated. Driving down litigation isn’t just about cutting costs to the NHS. It’s also about the patient: helping to improve their outcome, while protecting their dignity and quality of life.
Medstrom can offer a number of unique products to assist you in building a preventative care strategy. This includes our advanced fluid-immersion simulation surface Dolphin Therapy, as well as lateral tilt beds and cushions. Get in touch with the team today to find out more.
References
-
FOI #6883
-
FOI #6804
-
NHS (2017). Pressure Ulcer Productivity Calculator.
-
NHS Resolution (2022). Hospital acquired pressure ulcers and falls.
-
Tingle (2023). Clinical negligence litigation and the NHS: focusing on the injured patient. British Journal of Nursing. Accessed online on 18/12/2024.
-
Andah, B. Essang, C. Friend, et al. (2021). Understanding the impact of professional motivation on the workforce crisis in medicine: a rapid review. British Journal of General Practice (BJGP Open), 5(2).
-
Health and Social Care Committee (2022). Oral evidence: NHS litigation reform, HC 740. Q143. House of Commons.
-
H. Robertson, A. M. Thomson (2016). An exploration of the effects of clinical negligence litigation on the practice of midwives in England: A phenomenological study. Midwifery. Vol 33, p55-63.
-
Hibbs (1998). The Past Politics of Pressure Sores. Journal of Tissue Viability. 8(4).
-
NICE (2014). Pressure ulcers: prevention and management.
-
Care Quality Commission (2023). Taking action.